
![]()
Executive Summary
-
The Problem: A System-Demographic Mismatch. Penang is officially an “ageing society”, with 7.7% of its population aged 65 and over. Malaysia as a whole is quickly moving to become an “Ageing Nation” by 2029. Despite being recognized as an Age-Friendly City (AFC) by the World Health Organization (WHO), Penang’s key service systems remain disconnected. Health services, managed by the Federal government (MOH), and social care, managed by the State (JKM), operate in silos. This creates a “coordination gap,” which was a situation confirmed by an AFC stakeholder survey. The survey found a major disconnect where the service providers believe coordination exists while the community is “mostly unaware” of available services.
-
The Analysis: The Cost of Fragmentation. While often underestimated, this structural gap frequently leaves elderly patients and their families to act as their own care coordinators. This separation is a significant cause of costly, preventable hospital readmissions and reduced quality of life. Furthermore, this inefficiency places a burden on family caregivers and strains already limited healthcare resources. The current AFC framework represents a great vehicle for change, but a stronger mechanism is needed for proper integration. Its health-related actions (Domain 8) are treated as a separate project rather than a core approach to structurally connect existing Federal and State services.
-
The Solution: A Three-Part Roadmap. This paper proposes a three-part roadmap to build the missing connection: (i) Establish a high-level, state-led Penang Integrated Care Coordinating Body (PICCB), designed as a strategic Federal-State partnership to create unified care pathways and align leadership; (ii) Pilot a place-based “Integrated Care District” Model centred at the local Klinik Kesihatan and led by dedicated “Care Coordinators” to connect existing and separate services; and (iii) Invest in “Enabling Infrastructure,” specifically a shared digital care record system to overcome the critical 7% Clinical Information System adoption gap, targeted workforce training, and empowerment of enhanced AI in managing information from different sources.
By Dr. Tay Lyn Xuan (Visiting Researcher)1
1 Dr. Tay Lyn Xuan is currently a Postdoctoral Research Fellow at the Vanke School of Public Health, Tsinghua University, Beijing.
The Paradox of Progress: Penang’s Fragmentation Problem
The World Health Organisation has officially designated the state as a member in the Age-Friendly City (AFC) global network (see Appendix 1 & 2). [1][2] This is recognition of the existence in the state of strong political will and a solid framework for meeting the needs of an ageing population. However, alongside these developments lies a structural challenge: highly dependent senior citizens more often than not face a disjointed continuum of care. The services designed to support them are separated by different levels of government, technology, and information; this creates a “coordination gap” holding consequential risks to patient health integration and the state’s long-term finances.
The Demographic Collision Course
Penang is not just ageing; the rate of ageing is greater compared to the rest of the country. This places extra pressure on the existing healthcare system.
- With 7.7% of its population aged 65 and over, it has already crossed the 7% line to be considered an “ageing society”. [3]
- Projections show that by 2040, Penang will have the largest proportion of residents aged 60 and above in Malaysia, at 26.2%. [4]
- Most critically, Penang is projected to become the second state in Malaysia (after Perak) to become an “Ageing Nation” (defined as 15% of the population being 60 or over) by the year 2029. [5]
This 2029 projection creates a crucial timeframe for policy action. It means that the Penang state government’s goal to become an “age-friendly state by 2028” is not just an aspiration; it is a strategic necessity. [6] This means that the current healthcare delivery system will require structural adaptations to meet the long-term continuous care needs of an aging population. [7]
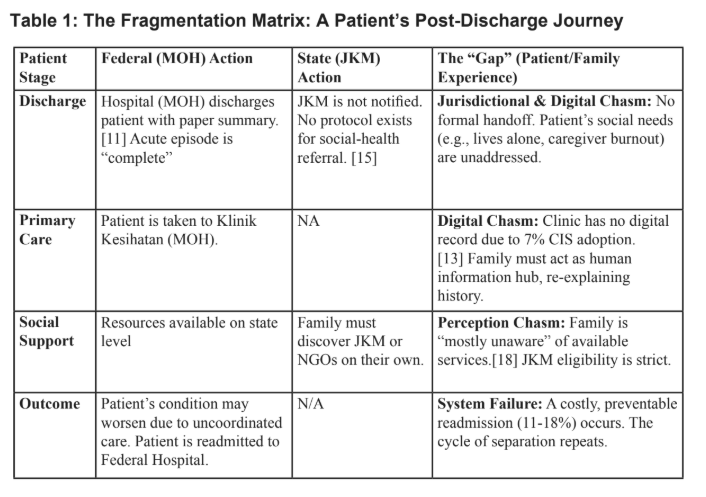
Acute hospitals, primary care clinics, rehabilitation centres, nursing homes, and home care services in Malaysia operate as separate entities with different funding mechanisms, information systems, and care philosophies. [8][9] For instance, when a 70-year-old patient is discharged from a federal-operated hospital after a critical medical event (like a stroke), the hospital’s care is considered completed after issuing a follow-up appointment at department clinics. [9][10]
The primary caregiver, who is usually a family member, is given a physical discharge summary, discharge medications and follow-up instructions. [11] At this point, the patient falls into a systemic gap defined by three distinct problems:
The Three Chasms of Coordination
1. The Digital Chasm
The hospital’s information system is currently not integrated to Klinik Kesihatan (health clinic) primary care centres. [12] Largely reliant on physical, handwritten medical records, the public primary health care network is still lagging in digitalisation, a challenge that is further compounded by an uneven infrastructure development. As of 2019, only 24% of public hospitals and 7% of all public health clinics in Malaysia were equipped with a Clinical Information System (CIS). [13]
This single statistic shows the physical reality of the coordination gap. It leaves the patient’s family to become an information hub, making the transfer of physical medical records from the specialist hospital to the local clinic their direct responsibility. At every step, they are required to do due diligence in visualising complex medical histories, which carries risks without sufficient health literacy. While the Ministry of Health (MOH) has pilot projects like HIS@KKM, these focus on MOH-internal processes and do not yet bridge the digital divide to the official departments of social care services. [14]
2. The Jurisdictional Chasm
The digital gap is exacerbated by jurisdictional boundaries, resulting in both systems operating in parallel. In addition, there is currently no formal integration process for the Federal hospitals (MOH) to notify the State-run social care system, the Jabatan Kebajikan Masyarakat (JKM), of a patient’s non-medical needs.
While the Ministry of Health (MOH) is responsible for health services under policies like the National Health Policy for Older Persons 2011, the State government is responsible for social welfare, providing institutional care and volunteer-based Home Help Services. [15][16] Also, while public healthcare institutions manage healthcare-related needs, the existing social system is not designed to handle the complexity of social-health referral and continuity of care. [16]
This fragmentation creates a substantial gap for patients who may not qualify for poverty assistance but still need essential social support to avoid compromising the household’s financial stability. Furthermore, even when families successfully navigate to JKM, they face strict eligibility criteria and long review durations. For instance, only 151,833 individuals, representing the 15% B40 segment, meet the stringent eligibility of receiving national support, where facilities are already limited. [17]
3. The Perception Chasm
The consequence of the digital and jurisdictional gaps is a “last mile” disconnect. A stakeholder outcome survey reported in an AFC policy brief [18] revealed widely differing views between service providers and the public. For instance, under policy area 3 (housing and infrastructure) and policy area 5 (social participation):
- Providers: State that services are “Mostly available.”
- The Community: State that they are “Mostly unaware of available government programmes.”
This survey finding reveals that the challenge is more than just a lack of services, but that low public awareness raises important issues regarding inter-level navigation at the community level. Even when social support is available, system fragmentation defaults the role of the care coordinator back to the family, increasing the strain to balance between work and care responsibilities. [19][20]
This fragmentation results in several pressing concerns:
- Patients face barriers in navigating the complex systems;
- Information rarely transfers fully;
- Preventive care is deprioritised in favour of more acute treatments; and
- Resources are concentrated in hospitals while community-based services remain underdeveloped.
Quantifying the Consequences
This structural disconnect has direct, measurable, and costly impacts on care delivery and the sustainability of public resources.
- Systemic Cost (Preventable Readmissions): Enhancing the coordination of post-discharge follow-up is an important step towards reducing costly and preventable hospitalizations. Malaysian national data shows that 11–13% of stroke patients are readmitted within 28 days [21] and 18% of heart failure patients are readmitted within 30 days, some of which are preventable. [22][23][25]
- Humanistic Cost (Caregiver Burden): These systemic gaps shift the burden of care onto the family. A Malaysian study on the societal cost of Alzheimer’s disease found it to be USD 8,618.83 per patient annually. A staggering 77.7% of this cost was attributed to informal care, constituting unpaid time, lost productivity, and burnout of the family. [24]
Consequently, the state’s healthcare system absorbs the cost of this, first through a revolving door of high-cost hospital stays, and second by shifting a substantial and often hidden burden onto families. This is not an isolated issue; it is the outcome of the current system’s operating framework.
CONTEXT AND PRECEDENTS: ACTIONABLE INTERNATIONAL MODELS
Addressing the challenge does not require inventing a new system from scratch, but rather adapting proven, practical principles from international models. By putting eyes on existing policies and care models from other countries, a blueprint for building the “engine” of integration that will greatly strengthen Penang’s AFC framework is possible to achieve.
What the AFC Gets Right (The Vehicle)
Penang’s existing AFC initiative has established a strong, multilevel governance structure that is critical for success [27]:
- Project Implementer: Majlis Bandaraya Pulau Pinang (MBPP)
- Project Manager: Penang Women’s Development Corporation (PWDC)
- Project Consultant: Malaysian Healthy Ageing Society (MHAS)
- This three-way partnership provides the vision, the political will, and, most importantly, a neutral platform [28] that is already supporting the necessary high-level dialogues between key State EXCO functions (such as Health and Social Development) and Federal officials (such as the State Health Director). [29]
The Critical Gap (The Missing Engine)
The AFC framework is the vehicle, but integrated care pathway is the engine. The framework’s primary gap is that its health-related component, Domain 8 (Community & Health Services), is treated as one of eight separate projects (alongside others like housing, transport, and social participation)[28]. While its current actions, such as community health campaigns or mobile apps, arevaluable, positive interventions at the community level and long-term resilience can be better achieved by aligning State (JKM) and Federal (MOH) health systems to create an integrated network of care for Penang’s aging population. [18][28] The AFC’s potential to support senior citizens in need, for instance, those requiring basic activity assistance or at risk of hospitalization, can only be fully realised once this structural gap is bridged.
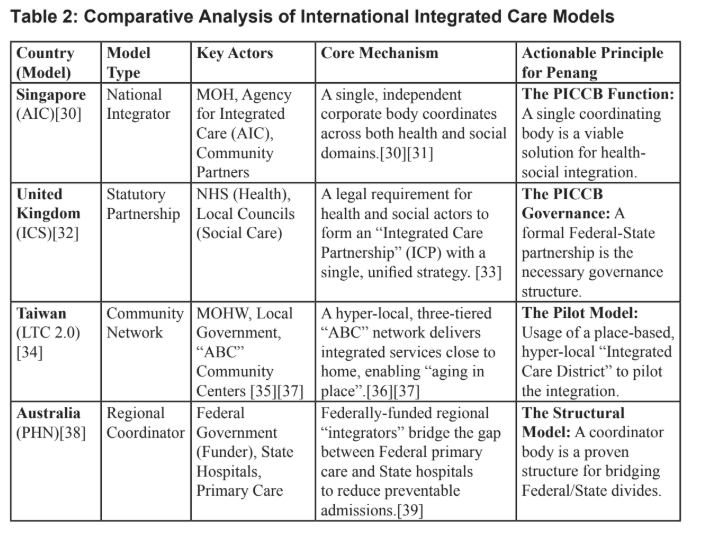
Actionable Principles from International Models
The following international models provide proven, practical principles for building our own integration engine.
THE WAY FORWARD: A ROADMAP FOR INTEGRATED CARE
The principle
This roadmap does not propose the creation of a new, expensive service delivery system. Instead, it uses the international principles from Table 2 to build the integration mechanism (the “engine”) that the existing AFC framework (the “vehicle”) currently needs. Hence, this is a proposed roadmap to connect existing assets and make the entire system function for high-needs seniors.
Establishing the “Penang Integrated Care Coordinating Body” (PICCB)
What it is: The PICCB would be a lean, high-level, state-led coordinating entity, not a new service provider. It is the “Penang version” of Singapore’s AIC [31] and Australia’s PHNs [38], designed to act as the central “integrator” for elderly care.
Governance (The UK Model): To be effective, the PICCB should be structured as a formal Federal-State partnership, adopting the principle of the UK’s ICS model. [33] This structure will function as a collaborative framework bridging the gap between state and federal jurisdictions.
- Leadership: The AFC’s potential for senior citizens in need (for instance, those requiring basic activity assistance or at risk of hospitalization) will be substantially achieved once this structural gap is bridged.
- Members: The board’s membership should involve leadership from JKM, as well as the core AFC implementers (MBPP and PWDC). [27][40]
Function (The AIC/PHN Model): The PICCB would function as a small technical office with three core functions:
- Map Pathways: Formally map unified care pathways for high-risk conditions (e.g., post-stroke, post-heart failure, neurological disorders or highly life-dependent conditions).
- Facilitate Integration: Act as the central authority to facilitate the data-sharing [41] and inter-agency barriers [15] from multiple public and private channels via mutual agreements.
- Monitor Outcomes: Be accountable for designing and monitoring system-level metrics, such as 30-day readmission rates, frequency of home help services per month, rate of successful application for long-term care institutions (RSK, RE), and caregiver satisfaction.
The PICCB would become the official implementation engine for Domain 8 of the Age-Friendly City plan [28], moving it from a “soft” campaign to a “hard” structural reform.
Pilot an “Integrated Care District” Model
What it is (The Taiwan/Australia Model): This roadmap proposes a place-based, hyper-local pilot, modelled on Taiwan’s community networks [36] and the regional focus of Australia’s PHNs [38]. This pilot would be centred around the catchment area of a single Klinik Kesihatan.
The Key Role: The “Care Coordinator”: This role provides the essential coordination needed to bridge current structural gaps.
- Role: A new dedicated position (e.g., a specially-trained nurse or social worker) based at the Klinik Kesihatan.
- Function: An alert is sent to this Care Coordinator upon hospital discharge. They evaluate social supports, discuss with caregivers, and tailor aid to real-world needs.
- A mobile healthcare team (doctors, nurses, pharmacists) conducts home visits for those with limited mobility (>5km radius).
- The PICCB develops a single, shared care plan as the family’s single point-of-contact.
- Connecting the Dots: Activates JKM HomeHelp services [42], connects to Senior Citizen Activity Centres (PAWE) [40], and refers to NGOs [43]. This directly addresses the “mostly unaware” perception gap.
- Mitigating Risk: To avoid “additional burden” [44], this must be a dedicated, funded position, not an extra task for existing staff.
Invest in Enablers: Digital & Workforce
Digital: A lean, cloud-based shared digital care record to address the 7% CIS adoption gap [13]. It allows the hospital, clinic, and coordinator to update the same care plan in real-time.
Workforce: Investment in formal training in resource management to professionalise the role and address the national shortage of elderly care professionals [46][47].
Enhanced AI: Task-specific LLMs can help the coordinator gather status updates and suggest care plans based on resource allocation, overcoming the digital chasm.
This is a High-Return Investment, not a New Cost
The cost of maintaining the status quo risks unsustainability. This framework is a proactive step towards long-term resilience:
- Elderly healthcare burden in Malaysia is projected to hit RM 21 billion by 2040. [46]
- Societal cost of Alzheimer’s is approx USD 8,600 per patient annually, mostly falling on families. [24]
Reducing preventable readmissions by even a few percentage points would generate savings that outweigh the funding requirements of the PICCB and Care Coordinators.
CONCLUSION: FROM AGE-FRIENDLY FRAMEWORK TO FUNCTION
With projections showing Penang becoming an “Ageing Nation” by 2029 [4][6], continuing a silo-ed system is both financially and socially unsustainable. [47] Penang may possess an excellent, WHO-recognized Age-Friendly Cities framework [1][2], but this report has argued that this framework currently lacks the functional procedures and infrastructure to bridge the divide between the Federal health (MOH) and State social care (JKM) systems.
This “coordination gap” is a critical systemic issue, evidenced by the visible “perception gap” among its citizens [18], high rates of preventable, costly hospital readmissions [22][23][25], and the overwhelming pressure placed on family caregivers. [26]
The three-part roadmap proposed in this paper provides an engine to make that framework function. With an integrated system in place, the current gaps can be further closed, and a patient’s journey to recovery can be made continuous and coordinated. The Federal-State gap can be bridged, and Penang’s goal of becoming an age-friendly state by 2028 [6] can become a functional reality for its most vulnerable seniors.
References
[2] WHO (2007). Global age-friendly cities: a guide.
[3] Penang population aged 65+. MBPP Official Portal.
[4] South China Morning Post, 2025. Malaysia’s states set to rapidly age.
[5] DOSM. Population Projections 2020-2060.
[6] Penang Gears Up To Become Age-friendly State By 2028 – bernama, https://www.bernama.com/en/news.php?id=2337919 [7] Thomas S, et al. Health care delivery in Malaysia: changes, challenges and champions. Journal of public health in Africa. 2011 Sep 5;2(2):e23. https://doi.org/10.4081/jphia.2011.e23 [8] Khor SK, et al. Sustainability and resilience in the Malaysian health system. Center for AsiaPacific Resilience and Innovation (CAPRI). 2024 Aug;2. https://www3.weforum.org/docs/WEF_PHSSR_CAPRI_Malaysia_2024.pdf [9] Ramli AS, Taher SW. Managing chronic diseases in the Malaysian primary health care–a need for change. Malaysian family physician. 2008 Apr 30;3(1):7. https://pmc.ncbi.nlm.nih.gov/articles/PMC4267020/ [10] Health White Paper for Malaysia – Ministry of Health Malaysia (2023) accessed November 21 2025. https://www.moh.gov.my/ [11] General Hospital Operational Policy – Kementerian Kesihatan Malaysia, accessed November 18, 2025. [12] Abd Razak N, et al. Investigating the barriers of health information system implementation in Malaysian Public Hospitals. IOP Conference Series. 2020. https://doi.org/10.1088/1757-899X/769/1/012054 [13] Naim N, et al. The evolution of healthcare digitalisation policies in Malaysia: A four-decade narrative review (1985–2025). Digital Health. 2025 Jul;11. https://doi.org/10.1177/20552076251353279 [14] Public Service Delivery and Local Government | eService Delivery | G2C | HIS@KKM, accessed November 18, 2025, https://www.malaysia.gov.my/portal/content/31329 [15] Malaysia’s Input For Cluster On Long-Term Care And Palliative Care, 9th Session Open-Ended Working Group On Ageing 2018. https://social.un.org/ageing-working-group/documents/ninth/Inputs%20Member%20States/Malaysia_LTC.pdf [16] Chan SL, et al. A review on family caregiving challenges in Malaysia. ProGCouns: Journal of Professionals in Guidance and Counseling. 2022. https://doi.org/10.21831/progcouns.v3i1.48386 [17] Laporan Tahunan 2022 – Jabatan Kebajikan Masyarakat Malaysia (2023). https://www.jkm.gov.my/ [18] Policy Brief: Age-Friendly City Penang Stakeholders Engagement Outcomes – Malaysian Healthy Ageing Society (MHAS). 2023. https://healthyageing.org/ [19] Sajali NS, et al. Lived experiences of Malaysian family caregivers of patients with chronic illnesses. Malaysian Family Physician. 2025. https://doi.org/10.51866/oa.683 [20] Availability and Burden of Family Caregivers in Caring for a Recurrent Stroke Survivor. The Malaysian Journal of Nursing (MJN). https://ejournal.lucp.net/index.php/mjn/article/view/1684 [21] Ang SH, et al. Risk of 28-day readmissions among stroke patients in Malaysia (2008–2015). PloS one. 2021. https://doi.org/10.1371/journal.pone.0245448 [22] Lim YM, et al. Trends for readmission and mortality after heart failure hospitalisation in Malaysia, 2007 to 2016. Global Heart. 2022. https://doi.org/10.5334/gh.1108 [23] Ziaeian B, Fonarow GC. The prevention of hospital readmissions in heart failure. Progress in cardiovascular diseases. 2016. https://doi.org/10.1016/j.pcad.2015.09.004 [24] Ong SC, et al. Annual societal cost of Alzheimer’s disease in Malaysia: a micro-costing approach. BMC geriatrics. 2025. https://doi.org/10.1186/s12877-025-05717-y [25] Glette MK, et al. Hospital physicians’ views on discharge and readmission processes: a qualitative study from Norway. BMJ open. 2019. https://doi.org/10.1371/journal.pone.0233457 [26] Lack of coordinated care for patients with long-term health issues – Healthcare Today (2025). https://healthcaretoday.com/ [27] Official Portal MBPP – Age Friendly City. https://www.mbpp.gov.my/ [28] AGE-FRIENDLY CITY – Resilient Cities Network. https://resilientcitiesnetwork.org/ [29] Connecting care across generations: WHO visits Penang, accessed November 18, 2025, https://www.who.int/ [30] Agency for Integrated Care (AIC) Singapore. https://www.aic.sg/ [31] Singapore’s Integration Solution – Istanbul Innovation Days. https://istanbulinnovationdays.org/ [32] Integrated Care Partnerships – UK LGA. https://www.local.gov.uk/ [33] What are integrated care systems? – NHS England. https://www.england.nhs.uk/integratedcare/ [34] Chen CF, Fu TH. Policies and transformation of long-term care system in Taiwan. Annals of geriatric medicine and research. 2020. https://doi.org/10.4235/agmr.20.0038 [35] Yeh MJ. Long-term care system in Taiwan: the 2017 major reform and its challenges. Ageing & Society. 2020. https://doi.org/10.1017/S0144686X18001745 [36] Long-term Care Plan 2.0 – Executive Yuan, accessed November 18, 2025, https://english.ey.gov.tw/ [37] Hung JY, et al. Analysis of Different Perspectives of Community-Based Long-Term Day-Care Centers. Int. Journal of Env. Research and Public Health. 2025. https://doi.org/10.3390/ijerph22071017 [38] Primary Health Networks (PHN) Australia. https://www.health.gov.au/our-work/phn/ [39] Booth M, et al. The new Australian Primary Health Networks: how will they integrate public health and primary care. Public Health Res Pract. 2016. https://doi.org/10.17061/phrp2611603 [40] WHO feature: Connecting care across generations: WHO visits Penang. https://www.who.int/westernpacific/newsroom/feature-stories/item/connecting-care-across-generations–who-visits-penang [41] Naim N, et al. Healthcare digitalisation policies in Malaysia. Digital Health. 2025. https://doi.org/10.1177/20552076251353279 [42] Empower support system for Elderly’s well-being – Bernama. https://www.bernama.com/ [43] PgCare Society One Stop Center. https://www.pgcarealliance.com/ [44] Foo CD, et al. Identifying key themes of care coordination for patients with chronic conditions in Singapore. Healthcare 2023. https://doi.org/10.3390/healthcare11111546 [45] Tun SY, Madanian S. Clinical information system (CIS) implementation in developing countries. 2023. https://doi.org/10.1093/jamia/ocad011 [46] Abdullah JM, et al. Healthy ageing in Malaysia by 2030. MJMS. 2024. https://doi.org/10.21315/mjms2024.31.4.1 [47] Haron SA, et al. Economic Burden of Healthcare Utilisation by Older Persons in Malaysia. JHPOR. 2024. https://doi.org/10.7365/JHPOR.2024.1.1
You might also like:
![Strengthening Malaysia’s Private Higher Education Sector through a Structural Revamp]()
Strengthening Malaysia’s Private Higher Education Sector through a Structural Revamp
![The Covid-19 Disruption Highlights the Neglected Nature of Arts and Culture Sector in Malaysia]()
The Covid-19 Disruption Highlights the Neglected Nature of Arts and Culture Sector in Malaysia
![Synergy among Stakeholders is Key to the Sustainability of Cultural Tourism in Penang]()
Synergy among Stakeholders is Key to the Sustainability of Cultural Tourism in Penang
![An Alternative Model of Skim Peduli Sihat to Pool Risks for B40 Households]()
An Alternative Model of Skim Peduli Sihat to Pool Risks for B40 Households
![George Town Heritage Celebrations: Achievements and Reflections]()
George Town Heritage Celebrations: Achievements and Reflections





